
I think the suspicion is that we export such trials so as to avoid potentially endangering our own population. I’m not sure that is justified, but that was my reading of the question.
A study started here (in Oxford, London, Southampton and Bristol) on Thursday just. Runs until May 2021.

Is it a valid concern or are there other reasons (genetic, for example) why testing in multiple areas of the world would be beneficial?


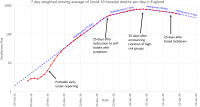





") ) we look a lot flatter in the tail of the "peak" so far...
) we look a lot flatter in the tail of the "peak" so far... 